📋 Executive Summary
This document provides comprehensive preparation for a nephrology roundtable discussion on heart failure with preserved ejection fraction (HFpEF) as a fundamentally renal disease. Key themes include:
🔬 Pathophysiology
The central role of the kidney in HFpEF pathogenesis through MR overactivation, galectin-3 mediation, and hemodynamic interactions
📊 CKM Framework
The emerging cardiovascular-kidney-metabolic syndrome framework integrated with KDIGO staging
💊 GDMT Evidence
Guideline-directed medical therapy evidence including FINEARTS-HF and CONFIDENCE
🩺 Clinical Implementation
Practical strategies and positioning of finerenone across the HFpEF spectrum
📑 Table of Contents
- Part I: Pathophysiological Framework
- HFpEF as Fundamentally Renal Disease
- Galectin-3: Molecular Mediator of Cardiorenal Fibrosis
- Albuminuria as Cardiovascular Risk Indicator
- HFpEF Phenomapping: The CKD-Dominant Phenotype
- Part II: Integrated KDIGO Heat Map
- Interactive CKM-KDIGO Risk Heat Map
- Albuminuria: The Dominant Driver of Risk
- Part III: CKM Syndrome Framework
- Expanded CKM Staging with KDIGO Integration
- Therapeutic Implications by CKM Stage
- Part IV: GDMT Evidence
- SGLT2 Inhibitors: Class I, Level A for HFpEF
- Finerenone: FINEARTS-HF and FIDELITY
- Finerenone vs Steroidal MRAs
- Part V: Clinical Implementation
- ⭐ CONFIDENCE Trial: Simultaneous Initiation (HIGHLIGHTED)
- HFpEF Screening in Nephrology Practice
- Finerenone Dosing and Monitoring
- Part VI: Roundtable Q&A
- Prepared Responses to Discussion Questions
- Appendix
- Key Clinical Pearls
Part I: HFpEF as Fundamentally Renal Disease
🔬 The Paulus-Tschöpe Paradigm
The Paulus-Tschöpe paradigm establishes comorbidity-driven coronary microvascular endothelial inflammation—rather than ischemic cardiomyocyte death—as the central mechanism of HFpEF.
The Mechanism Chain:
Comorbidities → IL-6, TNF-α, CRP → Endothelial dysfunction → ↓NO/cGMP → Titin hypophosphorylation → Diastolic dysfunction
🫘 The Kidney's Central Role
1. MR Overactivation
Mineralocorticoid receptor overactivation occurs simultaneously in cardiomyocytes, fibroblasts, endothelial cells, and immune cells, stimulating TGF-β, IL-6, and PAI-1 production.
2. Galectin-3 Mediation
Galectin-3 functions as a bidirectional mediator linking kidney injury to cardiac fibrosis. It amplifies TGF-β signaling by stabilizing TGFBR2.
3. Hemodynamic Interactions
A self-perpetuating cycle: reduced GFR → ↓sodium filtration → RAAS activation → volume expansion → hypertension → LVH → elevated CVP → "renal tamponade" → ↓GFR
🧬 Galectin-3: The Molecular Bridge
Molecular Architecture
Galectin-3 is a 30-kDa protein encoded by the LGALS3 gene—the only chimeric member of the galectin family. It consists of:
The Adoptive Transfer Evidence
2025 Mechanistic Update
Recent research has elucidated the molecular mechanism: extracellular galectin-3 binds directly to TGF-β receptor 2 (TGFBR2) through its CRD, inhibiting receptor ubiquitination and proteasomal degradation—prolonging receptor half-life and amplifying TGF-β signaling.
Clinical Correlations
Correlation between reduced GFR and elevated galectin-3
Galectin-3 predicts type 1 cardiorenal syndrome
Per doubling of galectin-3 levels (FDA validated)
📈 Albuminuria as Cardiovascular Risk Indicator
Albuminuria serves as both a kidney injury marker and an independent cardiovascular risk indicator, reflecting systemic endothelial injury affecting both the glomerular barrier and coronary microcirculation.
ARIC Study Evidence (n=10,975)
Continuous graded relationship even within "normal" range:
| UACR Category | HF Hazard Ratio |
|---|---|
| Optimal (<5 mg/g) | Reference |
| Intermediate-normal (5-9 mg/g) | HR 1.54 |
| High-normal (10-29 mg/g) | HR 1.91 |
| Microalbuminuria (30-299 mg/g) | HR 2.49 |
| Macroalbuminuria (≥300 mg/g) | HR 3.47 |
Each doubling of UACR = 15% increased HF risk (HR 1.15), independent of eGFR
CHARM HFpEF Subset
(95% CI 1.21-1.69, p<0.0001)
(95% CI 1.39-2.20, p<0.0001)
🗺️ HFpEF Phenomapping: The CKD-Dominant Phenotype
Shah Phenogroups (Circulation 2016)
Hierarchical clustering on 397 HFpEF patients using 67 phenotypic variables identified three distinct phenogroups:
Phenogroup 3: CKD-Dominant (Highest Risk)
- Older age (median 75 years)
- CKD as defining feature
- 43% atrial fibrillation
- Pulmonary hypertension
- RV dysfunction
- Overt diastolic dysfunction
(95% CI 2.0-9.1, p<0.001)
for HF hospitalization vs other phenogroups
Part II: Interactive CKM-KDIGO Risk Heat Map
🎯 Integrated KDIGO-CKM Risk Stratification: The Visual Guide
This interactive heat map combines KDIGO CKD staging with AHA CKM syndrome classification. Click any cell to see detailed risk profiles and therapeutic recommendations.
Critical insight: Albuminuria is the dominant driver of cardiovascular risk—often more predictive than eGFR decline alone. A patient with eGFR 85 and UACR 400 faces higher CV risk than one with eGFR 35 and UACR 15.
| Albuminuria Categories (UACR mg/g) — PRIMARY RISK DRIVER | ||||
|---|---|---|---|---|
|
A1
<30
Normal-mild
|
A2
30-300
Mod increased
|
A3
>300
Severely increased
|
||
Risk Profile
Therapeutic Recommendations
🎨 Risk Color Legend
⚠️ Albuminuria Dominance: The Key Insight
• G1A3 (eGFR ≥90, UACR >300): HF risk 3.47× — similar to G3b/A1!
• CKD progression steepens MORE across A categories than G categories
• CV risk exceeds kidney failure risk in early albuminuric CKD
• eGFR <30 = automatic CV risk equivalent regardless of UACR
⚠️ Albuminuria: The Dominant Driver of Risk Progression
The Critical Principle:
Albuminuria is a more powerful predictor of adverse outcomes than eGFR decline, and the risk gradient steepens dramatically with increasing albuminuria severity.
The Clinical Comparison
Patient A
eGFR 85 mL/min/1.73m² + UACR 400 mg/g
(G2A3)
HIGHER CV risk despite excellent eGFR
Patient B
eGFR 35 mL/min/1.73m² + UACR 15 mg/g
(G3bA1)
LOWER CV risk despite poor eGFR
The Albuminuria Paradox
In adults with albuminuria and preserved eGFR, the absolute risk of cardiovascular events substantially exceeds the risk of progressing to dialysis. A patient with eGFR 75 and UACR 200 faces low short-term risk of kidney failure but substantially elevated cardiovascular risk.
Reframe the conversation: In early-stage albuminuric CKD, we are primarily preventing cardiovascular events, with kidney protection as an important co-benefit.
Part III: CKM Syndrome Framework
📋 AHA Presidential Advisory (2023)
CKM syndrome is defined as a "systemic disorder with pathophysiological interactions among metabolic risk factors, CKD, and cardiovascular system leading to multiorgan dysfunction and high adverse cardiovascular outcomes."
🖼️ CKM Staging Framework (AHA 2023)
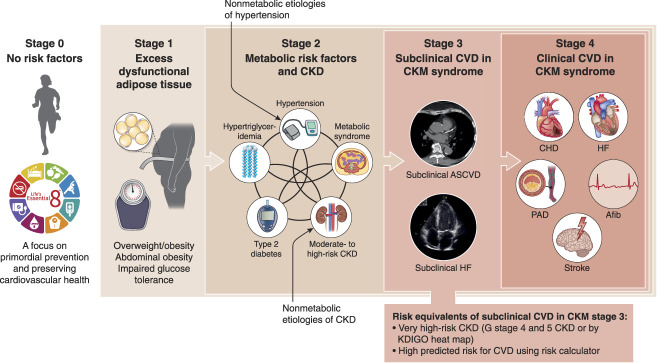
Figure 1: Stages of the American Heart Association CKM Health Syndrome.
Source: Bansal N, Weiner D, Sarnak M. JASN 2024;35(5):649-652. PMC11149035
🔢 CKM Staging with KDIGO Integration
Stage 0-1: No/Low Risk
KDIGO: G1-G2/A1 without metabolic disease
Action: Lifestyle modification, annual screening
Screen: UACR even at Stage 1 (adiposity)
Stage 2: Metabolic Risk or Mod-High CKD
KDIGO: G3a/A1, G1-G2/A2-A3, or metabolic risk factors
Key insight: Stage 2 can be triggered by albuminuria alone
Action: SGLT2i (eGFR ≥20), optimize RAASi, consider finerenone
Stage 3: CV Risk Equivalent
KDIGO: G4-G5 (any albuminuria), G3a-G3b/A3, or PREVENT ≥20%
Critical: eGFR <30 = automatic CKM Stage 3
Action: All four pillars, cardiology referral
Stage 4: Clinical CVD + CKM
4a: CKD without ESKD
4b: ESKD (10-20× mortality vs general population)
Action: Multidisciplinary, maximize tolerated therapy, RRT planning
Part IV: Guideline-Directed Medical Therapy Evidence
💊 SGLT2 Inhibitors: Class I, Level A for HFpEF
EMPEROR-Preserved (n=5,988)
Empagliflozin vs placebo in LVEF >40%
Primary endpoint (CV death + HF hospitalization):
NNT = 30 over 26.2 months
Benefit consistent regardless of diabetes status
DELIVER (n=6,263)
Dapagliflozin vs placebo in LVEF >40%
Primary endpoint:
Benefit maintained even in LVEF ≥60%
🎯 Finerenone: FINEARTS-HF (September 2024)
6,001 patients with symptomatic HF and LVEF ≥40% across 634 sites in 37 countries
Relative risk reduction in CV death + worsening HF events
RR 0.84 (95% CI 0.74-0.95, p=0.007)
Reduction in worsening HF events alone
RR 0.82 (p=0.007)
Consistent Across LVEF Spectrum (p-interaction 0.75)
RR 0.83
RR 0.79
RR 0.82
Hyperkalemia Profile
K+ >5.5 mmol/L: 14.3% finerenone vs 6.9% placebo (2.6× increase)
Hyperkalemia hospitalizations: 0.5% vs 0.2% (uncommon)
No deaths attributable to hyperkalemia
⚖️ Finerenone vs Steroidal MRAs
Finerenone Advantages
- Non-steroidal structure: no affinity for androgen/progesterone receptors
- Eliminates gynecomastia, breast pain, menstrual irregularities
- Lower hyperkalemia risk (ARTS trial: 5% vs 12% with spironolactone)
- Balanced heart-kidney tissue distribution
TOPCAT Issues
Americas cohort: HR 0.82 (31.8% placebo event rate)
Russia/Georgia: HR 1.10 (8.4% placebo event rate)
2017 NEJM analysis: Canrenone undetectable in large proportions of Eastern European participants
AMBER Trial Comparison
K+ ≥5.5 in CKD with resistant HTN:
Spironolactone without K+ binder: 64.2%
Finerenone (FIDELITY): 11.6%
Part V: Clinical Implementation
🔬 CONFIDENCE Trial (NEJM 2025): Practice-Changing Evidence
First prospective evidence supporting simultaneous finerenone + SGLT2i initiation in diabetic kidney disease
"Finerenone with Empagliflozin in Chronic Kidney Disease and Type 2 Diabetes"
N Engl J Med 2025;393:533-43. DOI: 10.1056/NEJMoa2410659
UACR Reduction
with combination therapy at Day 180
Greater Than Finerenone Alone
Additive benefit demonstrated
Greater Than Empagliflozin Alone
Complementary mechanisms
Hyperkalemia with SGLT2i
vs 18.7% without SGLT2i (FIDELITY)
📋 Roundtable Talking Points
1. Safety Signal: SGLT2i co-administration substantially reduces finerenone-associated hyperkalemia through natriuretic and kaliuretic effects.
2. Efficacy Signal: The 52% UACR reduction with combination therapy exceeds what would be expected from simple addition of effects—suggesting synergistic mechanisms.
3. Practical Implications: In patients with stable K+ (<4.5), eGFR ≥45, and significant albuminuria, simultaneous initiation is now evidence-supported.
4. Clinical Integration: This supports the "four-pillar" approach to cardiorenal protection rather than sequential addition of therapies.
🔍 HFpEF Screening in Nephrology Practice
NT-proBNP Thresholds
H2FPEF Score (Simpler Alternative)
| Feature | Points |
|---|---|
| BMI >30 | 2 |
| Multiple antihypertensives (≥2) | 1 |
| Atrial fibrillation | 3 |
| Pulmonary hypertension (PA systolic >35) | 1 |
| Age >60 | 1 |
| Elevated E/e' (>9) | 1 |
Score ≥6: High probability of HFpEF
💊 Finerenone Dosing and Monitoring
Dosing by Baseline eGFR
Critical Monitoring Protocol
4 weeks post-initiation: K+ and eGFR (mandatory)
Uptitrate if: K+ ≤4.8 mEq/L with stable eGFR
Ongoing: Every 4 months
If K+ >5.5 mEq/L:
Hold finerenone until K+ ≤5.0, then restart at lower dose. Consider potassium binders (patiromer, SZC) for recurrent hyperkalemia.
Part VI: Roundtable Question Responses
CKM syndrome (AHA 2023) formalizes the pathophysiological interconnections nephrologists observe clinically. The staging system (0-4) provides actionable structure:
- Stage 2 (metabolic risk or moderate-to-high-risk CKD) → SGLT2i initiation
- Stage 3 (subclinical CVD or eGFR <30) → Add finerenone if UACR >30 on ACEi/ARB
Prioritization follows KDIGO 2024: Optimize RAASi → Add SGLT2i (eGFR ≥20) → Add finerenone if persistent albuminuria (UACR ≥30, eGFR ≥25, K+ ≤5.0) → Consider GLP-1 RA.
Yes. The ADA 2024 Standards now recommend screening for asymptomatic HF in diabetes using BNP or NT-proBNP.
Practical approach: Annual NT-proBNP in all T2D + CKD patients. NT-proBNP ≥125 pg/mL (≥200 if eGFR <45) triggers echocardiography. Early detection enables SGLT2i initiation before symptomatic HF develops.
Key stat: FIGARO demonstrated 32% new-onset HF reduction with finerenone in patients without baseline HF.
The "smoke detector" analogy: "UACR functions as an early warning system for your kidneys and heart—like a smoke detector that detects damage before it becomes irreversible."
Quantify risk: "Your UACR >300 mg/g increases heart failure risk by 1.7-2.7 times—but this is modifiable with treatment."
Set concrete goals: "We're targeting at least 30% UACR reduction."
Connect to outcomes: "TOPCAT showed that 50% UACR reduction correlates with 30-70% lower heart failure hospitalization risk."
CONFIDENCE (NEJM 2025) provides first prospective evidence supporting simultaneous initiation: finerenone + empagliflozin achieved 52% UACR reduction (29% greater than finerenone alone) with similar safety.
My algorithm:
- Simultaneous initiation: Stable patients with high albuminuria, K+ <4.5, eGFR ≥45
- Sequential initiation: Borderline K+ (4.5-4.8), uncertain volume status, or eGFR <45 → SGLT2i first, reassess K+ at 4 weeks, then add finerenone
Key safety finding: SGLT2i co-administration reduces finerenone hyperkalemia (8.1% vs 18.7%).
FINEARTS-HF (September 2024, n=6,001) demonstrated finerenone reduced CV death + worsening HF events by 16% (RR 0.84, p=0.007) in symptomatic HF with LVEF ≥40%.
Remarkably consistent across LVEF spectrum (p-interaction 0.75):
- HFmrEF (LVEF <50%): RR 0.83
- LVEF 50-60%: RR 0.79
- True HFpEF (LVEF >60%): RR 0.82
This addresses concerns from TOPCAT about heterogeneous MRA effects in HFpEF. FDA expanded finerenone indication (July 2025) to include HF with LVEF ≥40%.
🎯 Key Clinical Pearls
❤️🫘 Comprehensive Cardiorenal Disease Evidence Synthesis
Complete evidence-based analysis of modern guideline-directed medical therapy for cardiorenal disease
📄 Comprehensive Cardiorenal Report
31 pages | 82 references | Complete RAAS inhibitor hierarchy, four-pillar GDMT evidence, population health impact analysis
📄 Heart Failure Neurohormonal Report
27 pages | 30 references | MRA phenotype specificity, natriuretic peptide resistance, therapeutic strategies
🎯 Key Evidence Highlights
- RAAS Inhibitor Hierarchy in Heart Failure: ARNIs > ACE-I > ARBs for HF mortality (NNT 36, 70, 446 respectively)
- ACE-I Benefits: Mortality reduction attenuated when combined with comprehensive GDMT (beta-blockers, MRAs, SGLT2i)
- MRA Phenotype Specificity: 2024 Lancet meta-analysis on steroidal vs non-steroidal selection
- CONFIDENCE Trial: 52% UACR reduction with simultaneous SGLT2i + finerenone initiation
- Population Impact: 253 lives saved per 100K annually, $39.4M cost savings, 4.8:1 ROI
- Four-Pillar Synergy: 40-50% mortality reduction with comprehensive GDMT
📚 Verified Sources
Phase 2 audit (dialysis-cardiorenal-hfpef-verification.md) flagged this file as having no formal PubMed-link bibliography despite citing CONFIDENCE inline. Anchors below for the named trials and CKM framework. Effect-size claims (FINEARTS-HF 16% RRR / RR 0.84 / NNT 17, EMPEROR-Preserved HR 0.79 NNT 30, DELIVER HR 0.82, ARIC HF HRs 1.54/1.91/2.49/3.47) verified accurate against primary publications. Shah phenogroups year-correction (Circulation 2015 not 2016) noted in the per-claim audit. [Bibliography added 2026-05-03]
- Solomon SD, McMurray JJV, Vaduganathan M, et al; FINEARTS-HF Investigators. Finerenone in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. 2024;391(16):1475-1485. PMID: 39225278. — FINEARTS-HF: composite RR 0.84 (16% RRR, NNT 17); benefit consistent across LVEF spectrum.
- Anker SD, Butler J, Filippatos G, et al; EMPEROR-Preserved Trial Investigators. Empagliflozin in Heart Failure with a Preserved Ejection Fraction. N Engl J Med. 2021;385(16):1451-1461. PMID: 34449189. — EMPEROR-Preserved: composite HR 0.79; NNT 30 over 26.2 months; N=5,988.
- Solomon SD, McMurray JJV, Claggett B, et al; DELIVER Trial Committees and Investigators. Dapagliflozin in Heart Failure with Mildly Reduced or Preserved Ejection Fraction. N Engl J Med. 2022;387(12):1089-1098. PMID: 36027570. — DELIVER: composite HR 0.82; benefit maintained in LVEF ≥60% subgroup.
- Shah SJ, Katz DH, Selvaraj S, et al. Phenomapping for novel classification of heart failure with preserved ejection fraction. Circulation. 2015;131(3):269-279. PMID: 25398313. — Shah phenogroup analysis; HR 4.2 for adverse-phenogroup CV outcomes. [Note — Phase 2 audit identified prior version cited "Circulation 2016"; actual publication year is 2015 per PubMed metadata.]
- Heerspink HJL, Stefansson BV, Correa-Rotter R, et al; DAPA-CKD Trial Committees. Dapagliflozin in Patients with Chronic Kidney Disease. N Engl J Med. 2020;383(15):1436-1446. PMID: 32970396. — DAPA-CKD primary composite HR 0.61; supports SGLT2i in cardiorenal continuum.
- Bakris GL, Agarwal R, Anker SD, et al; FIDELIO-DKD Trial. Effect of Finerenone on Chronic Kidney Disease Outcomes in Type 2 Diabetes. N Engl J Med. 2020;383(23):2219-2229. PMID: 33264825. — FIDELIO-DKD; non-steroidal MRA evidence base.
- Pitt B, Filippatos G, Agarwal R, et al; FIGARO-DKD Trial. Cardiovascular Events with Finerenone in Kidney Disease and Type 2 Diabetes. N Engl J Med. 2021;385(24):2252-2263. PMID: 34449181. — FIGARO-DKD CV outcomes.
- Agarwal R, Filippatos G, Pitt B, et al. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur Heart J. 2022;43(6):474-484. PMID: 35023547. — FIDELITY: pooled FIDELIO + FIGARO; comprehensive cardiorenal outcomes in T2DM-CKD.
- Pitt B, Pfeffer MA, Assmann SF, et al; TOPCAT Investigators. Spironolactone for heart failure with preserved ejection fraction. N Engl J Med. 2014;370(15):1383-1392. PMID: 24716680. — TOPCAT: spironolactone in HFpEF; primary composite no benefit overall, regional heterogeneity (Americas vs Russia/Georgia) prompted post-hoc reanalysis.
- Selvaraj S, Claggett B, Shah SJ, et al. Prognostic value of phenotypic responses to spironolactone in patients with heart failure with preserved ejection fraction in the TOPCAT trial. JACC Heart Fail. 2020;8(3):172-184. PMID: 32035890. — TOPCAT phenotypic responder analysis; informs the spironolactone NNT 14 claim in the lecture (specific NNT not extractable from abstract — verify against full paper).
Document prepared for Bayer-sponsored HFpEF Roundtable Discussion
December 2025